Methodology Introduction
First: Scope.
Second: Design.
Third: Organization.
Fourth: Data Collection.
Fifth: Disaggregation
Sixth: Review.
Seventh: Publication.
Eighth: Assessment.
Ninth: Managemen
The General Authority for Statistics (GaStat) applies in all its statistical work a unified methodology that conforms with the nature of each statistical product. It depends on the Handbook of Statistical Work Procedures, which is compatible with internationally approved procedures. Statistical products go through eight major stages, in addition to a ninth stage represented in the comprehensive “management” stage which is illustrated in the following figure and the subsequent explanations:
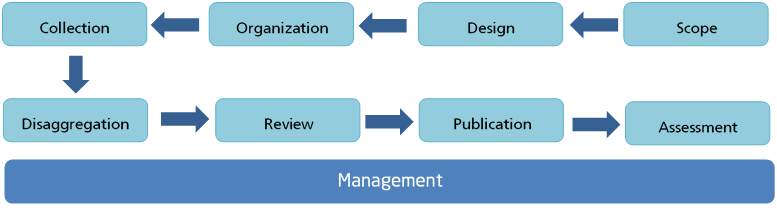
The first three stages (scope, design and organization) are collaborative stages between GaStat and its clients who are data users from development entities. The fourth stage (data collection) is a collaborative stage between GaStat and the statistical population, whether they are households or establishments, to complete data and information. The remaining stages (disaggregation, reviewing and publication) are statistical and are undertaken by GaStat. Afterwards, the eighth stage (assessment) is again done in collaboration with the clients. The management stage is administrative and organizational and spans all other stages. Those stages have been applied to the Household Health Survey as follows:
It is the starting point for producing the Household Health Survey. It is also the first collaborative stage between GaStat and a number of entities in the health sector in the Kingdom such as the Ministry of Health, the Saudi Health Council, as well as the private and academic sector. Workshops and meetings were held at this stage between the authority and those entities to reach a better understanding of their needs and know their requirements, given that they are the main beneficiaries of the Household Health Survey. The views of those entities are taken into consideration to ensure the attainment of all the objectives of the household health survey which are summed up as follows:
- Creating a database that could be used as a reliable source and reference to supply the international, regional and local organizations with the required health data and indicators.
- Providing statistical data that could help health planners to improve, update and monitor the implementation of some health policies and strategies.
- Providing statistical data that could enable health planners and decision makers to make international and regional comparisons in order to improve the competition in the health sector in Saudi Arabia.
- Providing statistical data that could help health planners to monitor and evaluate the implementation of some health programs, such as: programs that deal with chronic diseases, child mortality and fertility.
- Providing statistical data that could help in identifying those in need in order to support these segments of society with relevant initiatives and strategic health programs.
This stage also involves ensuring that the published statistics will contribute to meeting the requirements of Saudi Vision 2030 as well as covering regional requirements, such as the GCC Statistical Center, and international requirements represented in the World Health Organization.
Second Stage: Design:
This stage is for designing statistical work as an integrated product. It also includes identifying the statistical population, designing the statistical framework and the survey sample along with its questionnaire, identifying the method and tools of data collection and identifying the sampling units. Clients are made partners in all those procedures to benefit from their observations to meet all requirements and ensure that they are part of the statistical product.
The most important outputs of this stage are:
1. The Statistical Population:
The target statistical population of the Household Health Survey is composed of all individuals (Saudis and non-Saudis) who reside in Saudi Arabia.
2. Statistical Sources:
Data for the Household Health Survey Bulletin were collected using a field survey conducted periodically by GaStat every three years.
It is a household field survey conducted by GaStat and it falls under the category of (Education and Health Statistics). In this survey, data is collected by visiting a representative sample of households spread out across all administrative regions in the Kingdom of Saudi Arabia, and an electronic questionnaire containing multiple questions is completed. Estimates and indicators are consequently provided regarding the health status of members of the Saudi society in terms of the frequency of undergoing a periodic health examination, as well as indicators related to marriage, household planning, fertility and births, and the use of contraceptives for married women, in addition to indicators related to mortality rates, ..., and other indicators at the household level.
3. Household Health Survey Terminology and Concepts:
3.1 Administrative Region:
An administrative region is a part of Saudi Arabia that is run by a governmental agency affiliated to the Ministry of the Interior. In each administrative region there is a capital city. The kingdom is divided into 13 administrative regions.
All Saudi and non-Saudi individuals residing in the Kingdom at the time of the survey, as well as Saudi household members who are outside the country for education, trade, or tourism.
3.3 Survey population:
Household individuals who were selected as the sample unit including domestic helpers who live with them in the same dwelling.
Live birth is a fetus that exits the maternal body and subsequently shows any sign of life, such as: crying, breathing or heartbeats. The fetus is not considered alive if these signs did not occur, like what happens in abortion cases.
3.5 Exclusive breastfeeding:
Exclusive breastfeeding means that the infant receives only breast milk. No other type of feeding like formula milk is given.
3.6 Total fertility rate:
The average number of children that would be born to a woman over her lifetime if she were to live until the age of 50 and followed the same age-specific fertility rates.
3.7 Diagnosed chronic disease:
A diagnosed chronic disease is defined as a disease that has been diagnosed by a specialized doctor, by conducting the necessary tests for the individual and informing him/her of this chronic disease. This means that individuals who were not diagnosed by a specialist, whether they are aware of their disease or not, are not included in this definition.
3.8 Outpatient clinic visits:
When an individual visits a hospital or a health center to meet a doctor, and does not need to be admitted for overnight care.
3.9 Number of hospital admissions:
The number of times an individual has been admitted for overnight care in a hospital or healthcare center for a minimum of one night.
3.10 Infants:
Babies under one year of age.
3.11 Under-five children:
Children under five years of age.
3.12 Death:
The permanent disappearance of all signs of life (breathing, pulse, or voluntary movement) at any time after a live birth.
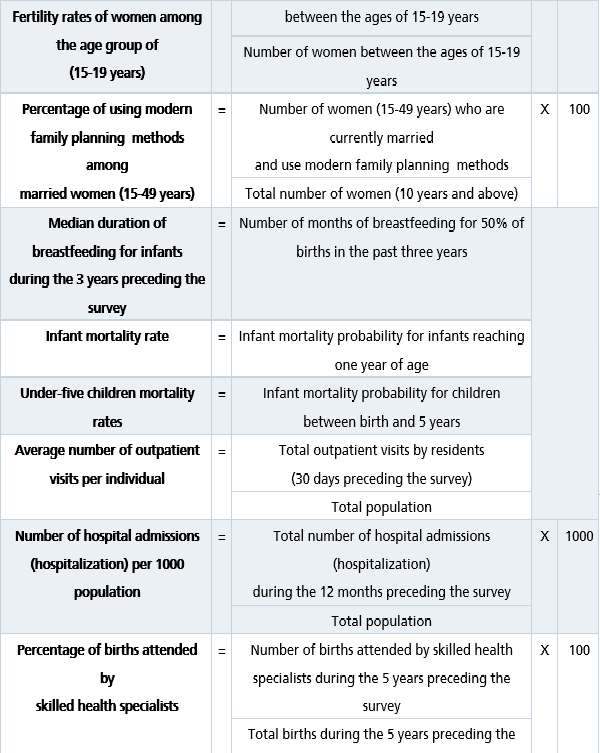
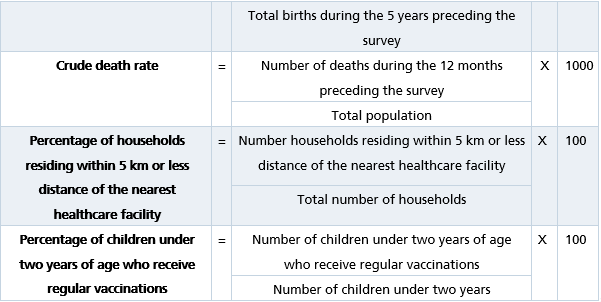
3.13 Indicators:
GaStat has adopted international standards for the calculation of household health indicators. These indicators are calculated according to the following equations:

3.14 Child mortality calculation methodology:
The direct method (as shown below) was used to calculate child mortality rates in the Household Health Survey of the Kingdom of Saudi Arabia for the year 1439 AH (2017). It is the same as the Demographic and Health Surveys (DHS) method implemented in many countries around the world with funding from the USAID. It is also the same multi-indicators cluster survey (MICS) method used by the United Nations Children's Fund (UNICEF) and the Pan Arab Project for Family Health (PAPFAM). This method allows full use of the latest data available during specific time periods.
The 2017 Household Health Survey questionnaire supplied the data required for using the direct method to calculate child mortality. This was achieved by creating a reproductive history table in which all live births were counted during the five years preceding the survey (including newborns living with their mothers during the time of the survey, newborns who do not live with their mothers in the same household during the time of the survey, and newborns whose mothers have died and are currently living with the household). Data has been collected regarding the gender; month and year of birth; survival rates; current age or age at death for all live births of mothers in the household.
A synthetic cohort life table approach has been used. This approach calculates age-specific probabilities of death by observing existing mortality data for past years. These probabilities are later grouped and sorted into common age groups that facilitate calculating child mortality.
By using these mortality probabilities, the following rates were calculated:
Infant mortality rates: The calculations are as follows:
First, the survival probability (p) was calculated for the following age groups:
0 months 1 = ( p0 ) - (Total deaths at the age of 0 months during the 5 years preceding the survey) / (Total live births at the age of 0 months)
1-2 months 1= ( p1-2 ) - (Total deaths at the age of 1-2 months during the 5 years preceding the survey) / (Total live births at the age of 1-2 months)
3-5 months 1= ( p3-5 ) - (Total deaths at the age of 3-5 months during the 5 years preceding the survey) / (Total live births at the age of 3-5 months)
6-11 months 1= ( p6-11 ) - (Total deaths at the age of 6-11 months during the 5 years preceding the survey) / (Total live births at the age of 6-11 months)
Second, survival probabilities for the age groups 0, 1-2, 3-5, and 6-11 months were multiplied:
= (p6-11)×(p3-5)×(p1-2)×(p0)
Under-five children mortality rates:
The calculations are as follows:
First, the survival probability (p) was calculated for all age groups as shown above:
Second, survival probabilities for the age groups multiplies 0,1-2,3-5,6-11,12-23,24-35,36-47,48-9 months:
= (p12-23) × (p24-35) ×(p36-47) ×(p48-59)
Third, under-five children mortality rates were calculated as follows:
= [1-(p0) ×(p1-2) ×(p3-5) ×(p6-11) ×(p12-23) ×(p24-35) ×(p36-47) ×(p48-59)] ×1000
3.15 Total fertility rate calculation methodology:
Total fertility rates are calculated by following the method used by the Demographic and Health Surveys (DHS) as well as the World Fertility Survey (WFS) by relying on the synthetic cohort method for women who have been married at a certain time period, and for specific age groups (15-49). Total fertility rate is defined as the average number of children that would be born to a woman over her lifetime if she were to live until the age of 50 and followed the same age-specific fertility rates. Total fertility rate has been calculated for the 3-year period preceding the survey.
The total fertility rate scope includes all women of childbearing age (15-49 years) and all births to these women during the 3 years preceding the survey.
To calculate the total fertility rate, the following steps are followed:
First, age-specific fertility rates are calculated for women who have been previously married among the following age groups :15-19، 20-24، 25-29، 30-34، 35-39، 40-44، 45-49 years, as follows:
Calculating the numerator:
It includes all births that took place during the 3-year period preceding the survey, for women who have previously been married, from each age group at the moment of birth distributed per time period and the mother’s age when the infant is born.
The time period (in months) is calculated by subtracting an infant's birth date from the date of the survey after converting both into what is known as the (Century-month code - CMC).
The mother’s age (in years) at the moment of childbirth is calculated by subtracting the mother’s birth date from the child’s birth date after converting both into what is known as the (Century-month code - CMC) and dividing the result by 60 and rounding it to full years.
Then the numerator (number of births) is allocated according to five-year age groups, which was formed according to the age of the mother when the child was born.
Calculating the denominator:
It includes the total (women person-years) i.e. years when women are likely to give birth, for all women in each age group during the 3 years preceding the survey distributed according to the mother’s age (divided into five-year groups) when the child was born. It is possible for women person-years to extend over two age groups).
Women person years (years when women are likely to give birth) were adjusted to include all women between 15-49 years old by multiplying the total women person-years for women who have previously been married (in each age group) by the All-Women-Factor for that age group.
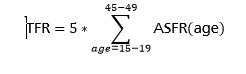
Age-specific fertility rates (ASFR) for all women = numerator/denominator
Total fertility rate (TFR) = 5 * (sum of the age-specific fertility rate for all age groups)
4. Adopted Statistical Classifications:
Classification is defined as being an arranged set of related categories used for data collection according to similarity. It is the basis for collecting and publishing data in all statistical fields, such as economic activity, products, expenditures, jobs or health, etc. It allows for classifying data and information through putting them into meaningful categories to produce useful statistics. Data collection requires a precise and methodological arrangement according to common features so that the statistics can be reliable and comparable. The Household Health Survey is subject to international standards in terms of collecting and classifying its data amd it uses the following guides and classifications:
4.1 Saudi classification for specializations and educational levels:
It is a statistical classification that is based on (ISCED) which is the reference for organizing educational programs and related qualifications based on the education levels and fields. It covers all the educational programs, levels and methods of learning as well as all educational stages starting from elementary school until higher education. This classification is used in the Household Health Survey to classify individuals aged 10 years and above according to their majors and education levels.
4.2 National guide for countries and nationalities:
It is an international and unified classification that covers countries and their affiliated territories, and is based on (ISO 3166) Country codes. The classification gives codes to countries and their affiliated territories. Using these codes and numbers instead of the country name is more beneficial for statistical purposes; as it saves time and limits errors. The purpose of using this classification in the Household health survey is to classify individuals according to their nationalities.
5. Design of Survey Questionnaire:
The survey questionnaire was drafted and designed by household health statistics experts at GaStat. International recommendations, standards, and definitions issued by the World Health Organization were taken into consideration during the design of the questionnaire, which was presented to household health experts and specialists, as well as to relevant entities to obtain their insights and comments. Questions were redrafted based on a specific scientific approach aimed at unifying question formats used by researchers.
The complete questionnaire can be viewed and downloaded through GaStat’s official website
https://www.stats.gov.sa/en/965
After being approved, the survey questionnaire will be transformed into an electronic questionnaire that can be handled through the advanced data collection system using tablet devices. The system has the following features:
- Reviewing the work zone of the field researcher (survey sample).
- Reaching the sample (household) using the map on the tablet device.
- Completing data of high quality using data check rules and navigation (to automatically detect input errors and illogical inputs while the completion of the data is underway).
- Establishing communication between supervising entities by exchanging notes with field researchers.
6. Coverage:
6.1 Spatial Coverage:
The Household Health Survey Bulletin covers data related to households for all 13 administrative regions of the Kingdom of Saudi Arabia, including: Riyadh, Makkah, Madinah, Qassim, Eastern Region, Asir, Tabuk, Hail, Northern Borders, Jazan, Najran, Al-Baha, and Al-Jouf. A scientifically selected sample representing the region’s households is visited in each region.
6.2 Temporal Coverage:
Data of the Household Health Survey in terms of the number of household members and their health characteristics are recorded as follows:
- Basic household member information in terms of numbers and main characteristics such as: Age, gender, nationality, educational level and marital status until the date of completing the questionnaire (the time of visiting the household).
- A member’s health status is recorded for a two-week period preceding the household visit.
- Data on infant mortality are recorded for a 5-year period prior to the household visit.
- Data on vaccinations are recorded for a 2-year period prior to the household visit.
- Data on outpatient visits are recorded for the (30)-day period prior to the household visit.
- Data on deaths are recorded for the year preceding the household visit.
7. Statistical Framework:
- The updated 2018 framework of the 2010 (1431H) Population and Housing Census Framework was used as a list containing all population items.
- The lists, maps and analytical standards of the units were set to choose data providers (households).
- The required descriptive data were identified in order to create the statistical framework, create the test framework, verify them, and use them for the current survey round.
8. Sample Design:
The survey population was divided into separate parts whose units are relatively homogenous. Each part was a layer, and each layer an independent population.
- Then, a random sample was selected independently from each layer. Finally, all sample units were combined to form the full unit.
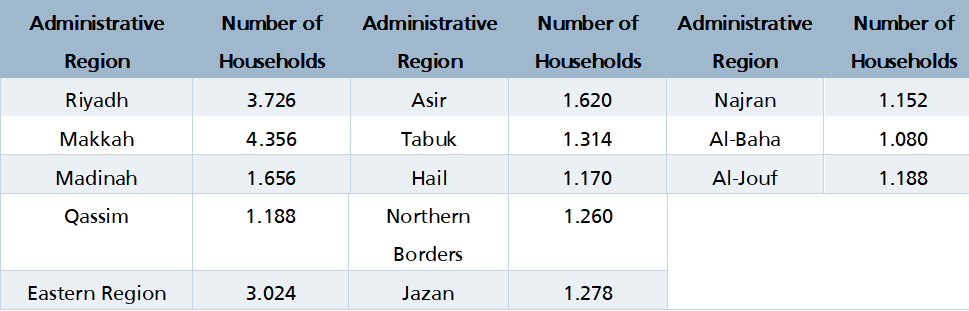
- The sample units were selected to cover the target statistical population. This step was carried out in two stages. In the first stage, the primary sampling units are selected, and these are the enumeration areas resulting from the process of coding and enumerating buildings and real-estate units. (1,334) enumeration areas were selected, and these areas are distributed across all administrative regions of the Kingdom by using a proportional size method and weighting the number of Saudi households. In the second stage, the final sampling units were selected, which are the households in the enumeration areas that were chosen in the first stage using the regular random sample. 18 households from each enumeration area were chosen, totaling (24,012) households at the level of Saudi Arabia.
- The optimal sample unit selection methodology was prepared with the aim of providing high-quality outputs with minimum burden on data providers using well-known statistical methods, such as rotation and controlling overlaps.
- The descriptive data required for establishing the statistical framework was selected and the sample was specified.
- The sample was then tested, evaluated, validated and used in the current survey round.
|
Sampling Units of the Household Health Survey: The basic sampling units are the enumeration areas. They are sampling units drawn in the first stage of designing the survey sample. Households are considered secondary and ultimate sampling units at the same time. They are sampling units drawn in the second stage of designing the survey sample. Each secondary sampling unit is considered a part of the basic sampling units. |
It is the final preparation stage preceding the visits to households and data collection. In this stage, the required workflow procedures are established for preparing the Household Health Survey, starting with the collection stage and ending with the assessment stage and the organization and grouping of such procedures. The optimal sequence of those procedures is chosen to arrive at a methodology that achieves the objectives of the survey. Those procedures were also described and documented to facilitate any updates to them in future rounds. The statistical workflow procedures were tested and examined to: ensure their compliance with the requirements of preparing the Household Health Survey in its final form, approve the procedures of the statistical workflow, and put a road map for implementation.
Testing the efficiency of input systems and the process of transmitting, synchronizing and reviewing data through either the tablet or office system of the household health survey are the main procedures in this stage.
Second: The workers who were nominated as field researchers and would later visit households to collect the household health survey data, were selected on the basis of several practical and objective standards related to the nature of the work, such as:
- Educational level.
- Fieldwork experience.
- Personal attributes, such as: good conduct, good senses and physical and psychological fitness.
- Candidate’s success in the training program of the Research and Development Survey.
- The candidate must not be under the age of 20.
Third: All candidates (GaStat staff and collaborators from some government entities) were qualified and trained through special training programs as follows:
- A training program was held for competent staff members in GaStat’s headquarters for one week.
- Similar training programs were held for collaborating inspectors, observers, and researchers from all the regions of Saudi Arabia.
|
The training programs offered to field researchers tasked with collecting the household health survey data include: Practical and hands-on lectures on technical, technological, administrative, and awareness materials that are used in data collection processes. Field researchers are also introduced to the survey’s objectives, the data collection method, and how to use maps and reach the holdings. The training programs also include a detailed explanation of all questions on the questionnaire, as well as any technical and administrative tasks. Field researchers are also trained on how to deal with the public and how to ask the questions in record time. At the beginning of the training program, all trainees are provided with tablet devices that enable them to do the following:
Staff members are nominated to participate in the survey based on their results that are automatically obtained from the “Trainees’ Automated Assessment System” to guarantee promptness, precision, and impartiality upon appointing the candidates and their competences. |
Fourth: Direct contact with the households was adopted as a method to fill the survey questionnaire and collect data. The field researchers visited the households listed in the survey sample and accessed them through coordinates on the tablets, guiding maps. Field researchers then introduced themselves, showing official documents proving their statistical identity. They also clarified the aim of their visit, and presented an overview of the survey and its objectives. The electronic questionnaire was then completed orally through direct contact with the head of the household or any adult member of the household who is familiar with its affairs.
Fifth: All field researchers use tablet devices to collect the survey questionnaire data according to timeframes specified for navigating the survey sections and the questionnaire items.
Sixth: Field researchers at all work locations in the Kingdom used the “synchronization” feature available on the tablet devices to download and transfer the completed data of the households directly to the database linked to them at GaStat’s headquarters where they are stored to be reviewed and processed at a later stage.
Seventh: Electronic check rules were applied to guarantee the accuracy, consistency, and rationality of the data entered in the household health survey questionnaire. They are electronic rules that identify contradictions and they were designed by using a logical link between the answers of the questionnaire and its variables to help field researchers directly identify any errors upon completing the survey data with the head of the household. Those programmed rules don’t allow any mistakes to go through when an answer contradicts with another piece of information or another answer in the questionnaire.
Eighth: The collected data is verified and reviewed by the field researcher, his/her inspector and the survey supervisor in the supervision area. All work areas are subjected to a monitoring and reviewing process from the Data Quality Room at GaStat’s headquarters. The room also controls and monitors the performance of all working groups in the field during the data collection process, from the first day and until the last day.
|
Data Quality Room: It is an operations room that works simultaneously with the field operations of the surveys. It is equipped with various electronic follow-up tools and monitoring and tracking screens. The observers and quality specialists in the room review the consistency of the data and detect errors and extreme values during the field data collection process. This is done by instantly and immediately following up on what is being completed by the field researcher to check the researchers’ commitment to the instructions of the survey, ensure the implementation of the schedule of arranged visits to the household or establishment, ensure the rationality and reliability of the data, and review some important survey indicators to ensure data accuracy. The room undertakes several tasks, mainly:
|
The disaggregation of the raw data of the Household Health Survey relies on the classification and coding inputs completed during the data collection process, whether they are classified based on the National Classification Guide for Countries and Nationalities which relies on (Country Codes - ISO 3166), the Saudi Classification for Specializations and Educational Levels which relies on (ISCED), or other classifications such as the distribution of data at the level of administrative regions, or qualitative and descriptive classification based on gender, or social status.
Data related to the Household Health Survey is displayed in suitable tables to facilitate summarizing, understanding and drawing conclusions from them, as well as comparing them to other data, observing statistical significance as they relate to the study’s population, and viewing data without the need to go back the original questionnaires. These tables contain data such as: The names and addresses of individuals in violation of the principle of statistical data confidentiality.
During this stage, specialists from the Department of Education and Health Statistics conducted data processing and analysis based on several procedures, as follows:
- Sorting and arranging data in a particular sequence or into different groups or categories.
- Summarizing detailed data into key points.
- Combining many data segments and ensuring their interconnection.
- Processing lost or missing data.
- Processing illogical data.
- Converting data into a form that has statistical significance.
- Organizing, presenting and interpreting data.
One of the most important data processing procedures that have been carried out is “data anonymization”. To ensure data confidentiality, GaStat removes identifiers from the input fields for the survey data, such as hiding the name and address of the head of the household and other identifiers to protect people’s privacy.
First: Verifying data outputs:
After reviewing and verifying the accumulated data of the household health survey, GaStat conducted at this stage processes of calculating and extracting results and uploaded and stored them on the database. The final reviewing processes were conducted by specialists in education and health statistics using modern technologies and software designed for the purposes of reviewing and checking.
Second: Handling of confidential data:
Pursuant to Royal Decree No.23 dated 07/12/1397, GaStat is committed to the absolute confidentiality of all completed data and not using them except for statistical purposes. Therefore, data are safely stored on GaStat’s servers. No individual data on households or any of their members shall be disclosed in any way. Materials set for publication are only aggregated statistical tables at the level of the Kingdom, the administrative regions and the major cities based on their features.
First: Preparing the results set for publishing:
In this stage, GaStat uploads data results from the Household Health Survey database. It then prepares publication tables and graphics for the data and indicators, and adds description and methodology information as seen in this Bulletin. These are prepared in both Arabic and English.
Second: Preparing media material and announcing the bulletin’s release date:
After announcing the bulletin’s release date on its official website at the beginning of the calendar year, GaStat prepares the required media materials to announce the bulletin’s release on all media outlets, as well as its various social media platforms. The announcement will be made on the date set for publication. The bulletin will be published on the official website in various templates of open data in Excel format which will be available on the website’s statistics library. This guarantees its circulation and access to all clients and parties interested in household health statistics.
Third: Communicating with clients and providing them with the bulletin:
GaStat pays great importance to communicating with clients who use its data. Therefore, GaStat contacts clients upon the release of the household health bulletin to provide them with it. GaStat also receives questions and enquiries from clients regarding the bulletin and its results through various communication channels. Clients can contact GaStat to request data. Questions and inquiries are received via:
- GaStat’s official website: www.stats.gov.sa
- GaStat’s official email: info@stats.gov.sa
- Client support email: cs@stats.gov.sa
- Visiting GaStat’s headquarters in Riyadh or one of its branches in the regions of the Kingdom.
- Official Letters.
- By Statistical Phone: (920020081).
GaStat’s Documents and Archives Center stored and archived the data of this bulletin to refer to it at any time upon request. GaStat took that step out of its awareness of the importance of electronically preserving this data to easily refer to it when needed.
After the results are released and received by GaStat’s clients, the clients are contacted again in this stage which allows for assessing the whole statistical process that was carried out, with the aim of constant improvement to obtain high-quality data. The improvements may include methodologies, processes, systems, statistical researchers’ skill and statistical frameworks. This stage is done in collaboration with data users and GaStat’s clients through a number of steps:
First: Collecting measurable assessment inputs:
Main comments and remarks are collected and documented from their sources at all stages, including those collected and documented during the collection stage, such as: comments and remarks presented by data collectors and their field supervisors, in addition to data collected and documented during the assessment stage such as the remarks deduced by specialists concerned with reviewing, checking and analyzing data collected from the field. Finally, comments and remarks presented by data users are collected and documented after publication, in addition to what is being monitored via media outlets or the clients’ remarks which GaStat receives through its main channels.
Second: Making the assessment:
Collected assessment inputs are analyzed, and on that basis a number of improvements and possible solutions are defined and discussed with concerned parties in all competent departments in the authority or its clients who are partners in the household health bulletin. This step also involves performance measurement of the clients’ use of the results of the household health bulletin and their satisfaction with them, contacting unsatisfied clients and providing them with clarifications.
On the basis of those procedures, an agreement will be made on the suggested recommendations to obtain high-quality data in the following round.
This is a comprehensive stage that covers all the stages of producing the Household Health Survey Bulletin. This stage determines the general production plan, including the feasibility study, risk management, funding, disbursement mechanisms, the development of performance indicators, quality parameters, the map of human resources needed for production, following up on the execution of tasks assigned to all departments in every stage, and the drafting of reports to ensure that GaStat fulfills its commitments towards its clients.